


 Sign Out
Sign Out


An additional 4 weeks treatment is recommended for patients in whom esophagitis has not healed or who have persistent symptoms.
Long-Term Management of Patients with Healed Esophagitis to Prevent Relapse: 20 mg once daily.
Symptomatic Treatment of Gastroesophageal Reflux Disease (GERD): 20 mg once daily in patients without esophagitis. If symptom control has not been achieved after 4 weeks, the patient should be further investigated. Once symptoms have resolved, subsequent symptom control can be achieved using 20 mg once daily. In adults, an on-demand regimen taking 20 mg once daily, when needed, can be used. In NSAID treated patients at risk of developing gastric and duodenal ulcers, subsequent symptom control using an on-demand regimen is not recommended.
Adults: In combination with appropriate antibacterial therapeutic regimens for the eradication of Helicobacter pylori and healing of Helicobacter pylori-associated duodenal ulcer, and prevention of relapse of peptic ulcers in patients with Helicobacter pylori-associated ulcers.
Esomeprazole 20 mg with amoxicillin 1 g and clarithromycin 500 mg, all twice daily for 7 days.
Patients Requiring Continued NSAID Therapy: Healing of Gastric Ulcers Associated with NSAID Therapy: Usual Dose: 20 mg once daily. The treatment duration is 4-8 weeks.
Prevention of Gastric and Duodenal Ulcers Associated with NSAID Therapy in Patients at Risk: 20 mg once daily.
Prolonged treatment after IV-induced prevention of rebleeding of peptic ulcers 40 mg once daily for 4 weeks after IV-induced prevention of rebleeding of peptic ulcers.
Treatment of Zollinger-Ellison Syndrome: Recommended Initial Dosage: 40 mg twice daily. The dosage should then be individually adjusted and treatment continued as long as clinically indicated. Based on the clinical data available, the majority of patients can be controlled on doses between 80-160 mg esomeprazole daily. With doses above 80 mg daily, the dose should be divided and given twice daily.
Impaired Renal Function: Dose adjustment is not required in patients with impaired renal function. Due to limited experience in patients with severe renal insufficiency, such patients should be treated with caution.
Impaired Hepatic Function: Dose adjustment is not required in patients with mild to moderate liver impairment. For patients with severe liver impairment, a maximum dose of esomeprazole 20 mg should not be exceeded.
Elderly: Dose adjustment is not required in the elderly.
Peprazom IV: Adults: Gastric antisecretory treatment when the oral route is not possible: Patients who cannot take oral medication may be treated parenterally with 20-40 mg once daily. Patients with reflux esophagitis should be treated with 40 mg once daily. Patients treated symptomatically for reflux disease should be treated with 20 mg once daily.
For healing of gastric ulcers associated with NSAID therapy the usual dose Is 20 mg once daily. For prevention of gastric and duodenal ulcers associated with NSAID therapy, patients at risk should be treated with 20 mg once daily.
Usually the intravenous treatment duration is short and transfer to oral treatment should be made as soon as possible.
Prevention of rebieeding of gastric and duodenal ulcers: Following therapeutic endoscopy for acute bleeding gastric or duodenal ulcers. 80 mg should be administered as a bolus Infusion over 30 minutes, followed by a continuous intravenous infusion of 8 mg/h given over 3 days (72 hours).
The parenteral treatment period should be followed by oral-acid-suppression therapy.
Impaired renal function: Dose adjustment is not required in patients with impaired renal function, Due to limited experience in patients with severe renal insufficiency, such patients should be treated with caution.
Impaired hepatic function: GERD: Dosage adjustment is not required in patients with mild to moderate liver impairment. For patients with severe liver impairment, a maximum daily dose of 20 mg Esomeprazole should riot be exceeded.
Bleeding ulcers: Dose adjustment is not required In patients with mild to moderate liver impairment. For patients with severe liver impairment, following an Initial bolus dose of 80 mg Esomeprazole for Infusion, a continuous intravenous infusion dose of 4 mg/h for 71.5 hours may be sufficient.
Elderly: Dose adjustment Is not required In the elderly.
Pediatric population (children and adolescent aged 1-18 years): Gastric antisecretory treatment when the oral route Is not possible: Patients who cannot lake oral medication may be treated parenterally once daily, as a part of a full treatment period for GERD (see doses in table as follows).
Usually the intravenous treatment duration should be short and transfer to oral treatment should be made as soon as possible.
Recommended intravenous doses of Esomeprazole: (See Table 2.)
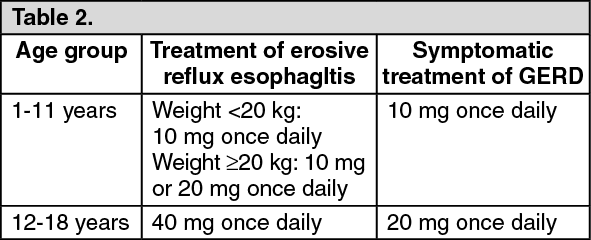 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdministration: Peprazom: The capsules should be swallowed whole with liquid. The capsules should not be chewed or crushed.
For patients who have difficulty in swallowing, the capsules can be opened and their content dispersed in ½ a glass of non-carbonated water. No other liquids should be used as the enteric coating may be dissolved. Stir and drink the liquid with the granules immediately or within 30 mins. Rinse the glass with ½ a glass of water and drink. The granules must not be chewed or crushed.
For patients who cannot swallow, the content of the capsules can be dispersed in non-carbonated water and administered through a gastric tube. It is important that the appropriateness of the selected syringe and tube is carefully tested.
Through Gastric Tube: 1. Add the contents of a capsule into approximately 25 mL or 50 mL of water (for some tubes, dispersion in 50 mL water is needed to prevent the granules from clogging the tube). Stir.
2. Draw the suspension into a syringe and add approximately 5 mL of air.
3. Immediately shake the syringe for approximately 2 min to disperse the granules.
4. Hold the syringe with the tip up and check that the tip has not clogged.
5. Attach the syringe to the tube whilst maintaining the above position.
6. Shake the syringe and position it with the tip pointing down. Immediately inject 5-10 mL into the tube. Invert the syringe after injection and shake (the syringe must be held with the tip pointing up to avoid clogging of the tip).
7. Turn the syringe with the tip down and immediately inject another 5-10 mL into the tube. Repeat this procedure until the syringe is empty.
8. Fill the syringe with 25 mL of water and 5 mL of air and repeat step 6 if necessary to wash down any sediment left in the syringe. For some tubes, 50 mL water is needed.
Peprazom IV: Injection: 40 mg dose: 5 ml of the reconstituted solution (8mg/ml) should be given as intravenous injection over a period of at least 3 minutes,
20 mg dose: 2.5 ml or half of the reconstituted solution (8mg/ml) should be given as an intravenous injection over a period of approximately 3 minutes. Any unused solution should be discarded.
10 mg: 1.25 ml of the reconstituted solution (8mg/ml) should be given as an intravenous injection over a period of at least 3 minutes. Any unused solution should be discarded.
Infusion: 40 mg dose: The reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes.
20 mg dose: half of the reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes. Any unused solution should be discarded.
10 mg dose: a quarter of the reconstituted solution should be given as an intravenous infusion.
80 mg bolus dose: The reconstituted solution should be given as a continuous intravenous infusion over 30 minutes.
8 mg/h dose: The reconstituted solution should be given as a continuous intravenous infusion over a period of 71.5 hours (calculated rate of infusion of 8 mg/h).